
Infants and young children have little respiratory reserve and can develop respiratory failure and hypoxemia quickly when they are ill.
The infant metabolic rate is roughly double the adult rate. Full-term infants are born with 20 million to 50 million alveoli, about 10% of the 200 million to 500 million found in the adult—giving them about 26 times less area for gas exchange. Surface area varies from 2.8 m2 in the infant (about the size of a baby blanket) to 75 m2 in the adult (about half a tennis court).
Regardless of age, a normal resting tidal volume (TV) is about 8 mL/kg of lean body weight. A 2.7-kg infant’s TV is only about 22 mL. Functional residual capacity (FRC), the amount of air left in the lung after a normal exhalation, effectively acts as the lung’s oxygen tank. The larger the FRC, the bigger the oxygen tank and the more respiratory reserve. FRC in an adult is about 70 mL/kg and is about 18 mL/kg in the infant. With a 75% smaller oxygen tank, the infant can’t hold his breath as long as an adult.
Dead space is also higher in the infant (3 compared with 2 mL/kg in the adult). A larger dead space means less of the TV is available to ventilate alveoli and more of each breath is wasted.
Putting all these values together, Figure 1 demonstrates the profound differences in the lung volumes that affect ventilation of a 2.7-kg infant compared with a 60-kg adolescent. The infant or toddler must have a higher respiratory rate and heart rate to compensate for smaller TVs, larger dead space, higher oxygen consumption, and higher carbon dioxide production. Slow respiratory or heart rate can rapidly lead to cardiorespiratory failure. The smaller TVs of an infant and a toddler also increase the risk for barotrauma when they are exposed to large TVs or high inflation pressures.
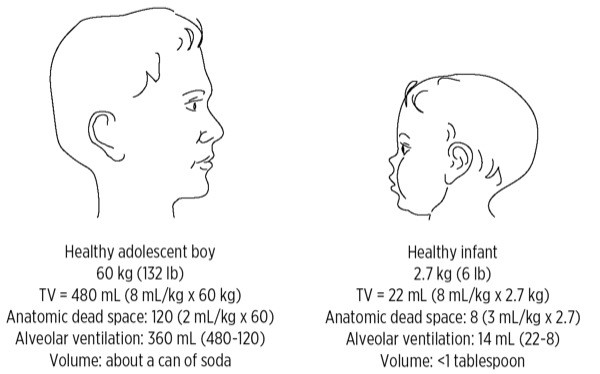
Figure 1
TV must be appropriate for the size of the child to ventilate adequately and avoid barotrauma. Anatomic dead space also has a great impact on whether a particular TV provides adequate alveolar ventilation. TV (tidal volume)
The pediatric chest wall is mechanically less efficient and limits potential lung expansion. Babies “belly breathe.” To take a deep breath, the infant’s chest can only expand a little because of the more horizontal angles of the rib cage. The abdomen therefore expands a lot as the diaphragm descends, pushing abdominal contents down and out of the way. Anything that interferes with descent of the diaphragm, such as a stomach or intestines distended with air or liquid, can seriously impair an infant’s breathing.
The infant’s chest wall is also more compliant than an adult’s, with an elastic recoil close to zero because of the lack of rib cage ossification. When the infant takes a breath against resistance, such as with airway obstruction or poor pulmonary compliance from pneumonia, the chest wall actually moves inward as the belly moves outward. The inward movement of the chest wall decreases the amount of air that enters. A rocking chest wall motion is very common in children who have even partial airway obstruction.
Because chest wall structure and belly breathing limit the ability to increase TV, the infant must rely on increases in respiratory rate to compensate for respiratory distress. The harder a child tries to breathe; the less efficient and more labored breathing becomes (Figure 2).
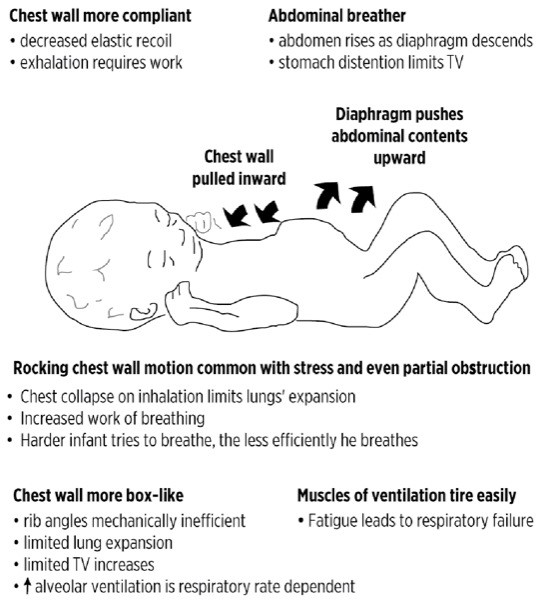
Figure 2
The mechanics of infant and toddler breathing increase the risk for respiratory failure. TV (tidal volume)
If your patient is not breathing well after opening the airway, then you must assist by using a technique appropriate for the age of the child.
Preoxygenate All Patients If Possible
Optimize oxygenation. If the child won’t tolerate the mask, use blow-by oxygen. If you’re not sure of the airway, use 100% oxygen for induction. If I choose to use nitrous oxide to assist an induction, I never use more than 50% and then will turn off the nitrous oxide once the child falls asleep in order to maximize preoxygenation.
Minimize Apneic Periods
During elective anesthesia, and in the absence of preoxygenation, hypoxemia can occur rapidly—even in the brief period between stopping mask ventilation and insertion of an LM airway or ETT. If you must interrupt ventilation, use apneic oxygenation by holding the airway open while administering oxygen by face mask.
Obtain a Good Mask Fit
To ventilate a child, first choose the correct mask size. The proper size covers the space between the bridge of the nose and the crease of the chin. Too large or too small a mask will prevent a good seal.
The face of an infant or a toddler is a lot smaller relative to your hand. You will still use your thumb and forefinger to press the mask against the face. Unlike in the adult, however, the size of your hand may not allow you to put all your fingers on the mandible. It’s not uncommon in a small infant to use just your third finger on the jaw to pull the face into the mask, with the fourth and fifth fingers free. Don’t press on the soft tissue under the chin with the remaining finger(s). Pressure there can increase airway obstruction by pushing the tongue and epiglottis back over the laryngeal outlet, and by compressing the soft laryngeal cartilages (Figure 3A and B).
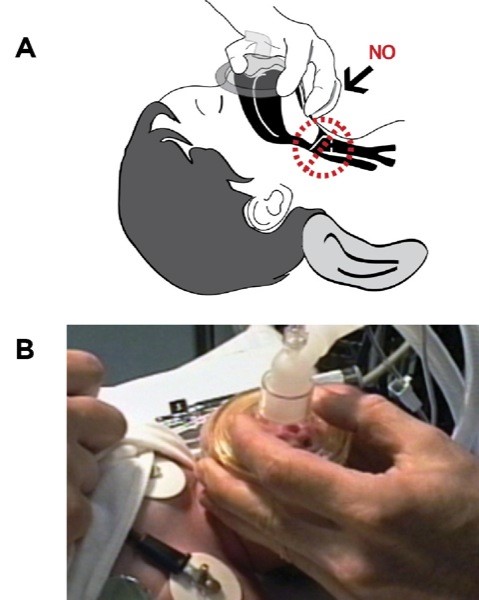
Figure 3
A. Keep your fingers on the bone, not the soft tissue under the chin, to avoid obstructing the airway. The provider may choose to keep the fourth and fifth fingers free. B. Note third finger on mandible, fourth and fifth fingers avoid pressure over larynx.
Note: Pictures intended to be conceptual; sterile gloves are required.
Protect the eyes since small face size, large eyes and a minimal bridge of the nose place the child’s eyes in harm’s way from the mask. Consider taping them closed before applying the mask if the patient is unconscious.
It is essential that you know the appropriate size of your child’s TV. An infant weighing 3 kg has a 24-mL TV (8 mL/kg × 3 kg), which is less than 2 tablespoonfuls (30 mL). A 70-kg adult has a 560–mL TV. Because the walls of a child’s lungs are thinner and less mature, they are more fragile and more easily damaged. Giving an adult-sized TV to a small child can overpressurize the lungs and cause pneumothorax.
If you can, choose a ventilation bag appropriate for the size of the child. It is easier, and safer, to deliver a 30-mL TV when using a 250-mL infant bag than a 1-L adult bag.
Always watch the chest expand while ventilating to estimate the size of the TV you are delivering. Ensure the airway is open to avoid stomach distention, which can seriously impair your ability to ventilate a baby. If the diaphragm can’t descend, then air can’t easily enter the lungs. If stomach distention occurs, then pass a soft suction or oral gastric tube to decompress. You will often see marked improvement in ventilation.
Case: One of my colleagues, a skilled anesthesiologist who infrequently anesthetizes small children, had just done a mask induction on an 18-month-old boy weighing 11 kg for hypospadias repair. I was assisting as an extra pair of hands by starting the IV line. After he intubated the patient, he pressed the start button on the ventilator. I looked over at the ventilator as he did so and saw the ventilator was set to volume mode and the tidal volume was still at the 500-mL default setting for an adult. Unable to reach the ventilator itself, I quickly disconnected the breathing circuit from the ETT and pointed out the problem. The baby never got the first breath. We were lucky.
Anesthesia providers often rely on the safety features of modern anesthesia machines, such as the high-pressure alarms, to help protect patients. However, you must take extra precautions when using your anesthesia machine on a child because there is little margin for error. What could be an inconsequential mistake in an adult can be a catastrophic error in a baby.
Use Pressure Mode Instead of Volume ModeEven though you can use either pressure control mode or volume control mode to ventilate a child, it is more common to use pressure control. Historically, older anesthesia machines lacked the precision to deliver the small TVs needed to ventilate a small baby. In addition, the provider would not know whether the TV chosen would deliver too high of an inspiratory pressure until after the first breath or two had already been delivered.
By using pressure control mode, the provider can deliver very small TVs with a preset maximum pressure, thereby avoiding potential overpressurization of the circuit and barotrauma. By starting with a lower than anticipated set pressure, you simply watch how the chest expands as you slowly, and safely, increase inspiratory pressure until the optimal TV is achieved. If you don’t see the chest expand, the TV is too small. I always watch my patient’s chest when setting the ventilator to verify that my patient is ventilating optimally.
Always Preset the Maximum Pressure And Tidal VolumeStarting an anesthesia machine ventilator for an adult patient is sometimes done in a very spontaneous manner. By this I mean the ventilator is often started using the default 500-mL TV setting. The provider then modifies the TV setting after the first few breaths for that particular patient. If you are caring for an average-sized adult, you will rarely cause harm with this technique. However, if you deliver a 500–mL breath to your 5-kg baby (40-mL TV) or 15-kg toddler (120-mL TV), you could very well cause a pneumothorax with the first breath.
Use your machine’s neonatal or pediatric settings. Always preset your ventilator settings for the size of the child you’re going to ventilate. Do so even if you plan spontaneous ventilation, because your anesthetic plan could change quickly.
Even when I am going to use the pressure control mode, I always preset my volume control parameters, too. In an emergency, or any moment of distraction, it’s too easy for you—or anyone who comes to help you—to accidentally turn on the volume mode instead of the pressure mode. If you’ve left the machine with any default adult settings, accidentally turning on the wrong mode could be dangerous.
Watch Your Pop-Off Valve to Avoid BarotraumaTo avoid traumatizing a child during elective surgery, anesthesia providers often perform a mask inhalational induction. It’s very common during mask inductions to use high volume flow, even a 10-L per minute flow, to rapidly change the agent concentration.
Once a patient is intubated, the ETT is immediately attached to the breathing circuit. Failure to fully open the pop-off, or to decrease the flow, can distend the ventilation bag and lead to potential barotrauma. The rather humorous picture in Figure 4 is an anesthesia machine inadvertently left in test mode for several minutes, with the pop-off valve set to 20 mm Hg and 10-L flow. Technically 20 mm Hg is not that high a pressure, but I think we can all agree that the ventilation bag is distended to the extent that if this were a pair of lungs, there might be serious trauma.
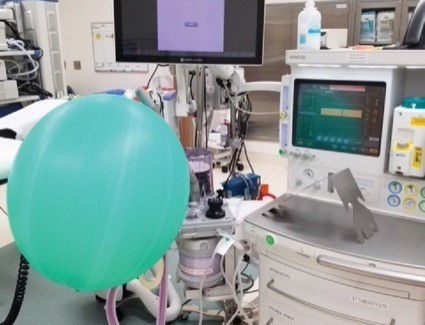
Figure 4
Anesthesia machine inadvertently left in test mode with high flow and 20 mm Hg pressure on pop-off valve.